
{kind=link}
An interesting comment
An interesting comment was left in a previous article about a video made by a contrarian doctor. According to reader named Squirrelelite, this doctor,
Mentioned a tweet from Matthew Yglesias suggesting that lots of people would have died if we had waited to do an RCT to approve boosters as Gruber and Krause wanted. He then goes on to claim that 2 or 3 hundred thousand people would have quickly signed up for the trial to get access to a booster shot, ignoring the huge cost and time delay to enroll 5-8 times as many people as were in the original vaccine trials. And he states that it would “only” take 11 months to run that trial. He claims we don’t have effectiveness results on 12-15 year olds without such a trial and also ignores these results from back in February or this result from January… (He) claims Gruber and Krause were “vindicated” but he doesn’t talk about any numbers to support that.
I confess, I lacked the fortitude to watch the video Squirrelelite provided, so I can’t promise they are reporting it fairly. Regardless, it’s certainly true that many doctors have lamented that boosters – and multiple other pandemic interventions – have not been studied in large, randomized controlled trials (RCT). Squirrelelite’s comment referenced Drs. Marion Gruber and Philip Krause, two scientists who resigned from the FDA last summer in protest of the decision to offer a booster to all adults. They felt there was not enough evidence to support this. They shouldn’t be called anti-vaccine for their skepticism of boosters at the time, but they haven’t exactly been vindicated, as I will explain.
Having an idea for an RCT is infinitely easier than actually doing an RCT
I love RCTs. All doctors do. In a fantasy world with unlimited time and money, but without ethics, an RCT would yield the optimal answer for many medical questions. They are the gold-standard for their ability to randomize patients and minimize bias. They are truly a remarkable achievement with a fascinating history. I firmly believe that every intervention that can be studied via an RCT should be.
However, in the real world, significant ethical and practical limitations prevent us from doing this. Having an idea for an RCT is infinitely easier than actually doing an RCT.
- The safety of the subjects in RCTs is paramount, as it should be, especially given the history of Nazi atrocities and the Tuskegee Study. Basic ethics and Institutional Review Boards (IRBs) strictly limit what can be studied via an RCT. RCTs can only be used to study interventions that have a reasonable chance of benefiting patients or when there is true uncertainty about which treatment is better, which is termed clinical equipoise. There’s never been or will be an RCT showing that smoking harms or that parachutes help. Having said this, there are many fewer “parachutes” in medicine than we often believe. Medicine is full of treatments that everyone “knew” worked, until they were found to be useless in an RCT. To repeat, I firmly believe that every intervention that can be studied via an RCT should be.
- Only the largest RCTs can reliably detect rare treatment harms or benefits. The rarer the event, the larger a study must be to detect it, something termed a study’s power. Generally, rare events can only be detected once the studied treatment has been given to large numbers of people outside an RCT. Real-world studies have taught us much more about rare vaccine harms and benefits than the RCTs.
- RCTs are hard to do for rare diseases as it is challenging to enroll enough patients.
- RCTs are of relatively short duration. Any treatment harm or benefit that occurs many years later is unlikely to be detected via an RCT.
- RCTs are slow. A doctor who has an idea for an RCT can’t just start one the next day. It takes time to design the trial, to get funding, to have it evaluated and approved by an IRB, to set up the infrastructure, to enroll patients, to run the study, and to synthesize the data. Most RCTs take many years to from the time they are conceived to when the final data changes clinical care, which is obviously problematic in a pandemic that arrived like a tornado. As I will discuss, the COVID vaccine trials had several unique features, including the rapid spread of COVID, that allowed them to proceed faster than most RCTs.
- RCTs are expensive, and funding can be hard to come by, especially for studies where no one can profit based on the outcome. The COVID vaccine trials were unique in that full funding was immediately available.
- An RCT can sound perfect right until the moment you actually have to enroll patients into it. Those of us who have done this know that recruitment can be very difficult. Some patients are eager to do so, but many don’t want to be a “guinea pig”. A normally hard process is much harder in a pandemic. One researcher, who has actual experience running an RCT this pandemic, said:
I think of what my clinical research team went through to enroll people in that trial, and I thought my nurses were going to die. One of them got covid and got sick. Imagine trying to do that on a daily basis, multiple patients, some of them facing intubation, none of them have their families
Patients or their families have to be able to give informed consent, which can be impossible for delirious, intubated COVID patients and their distraught families. As another researcher said:
There was one day our system had 84 deaths. And then you’re going to ask me to potentially put them on a placebo? It’s just really heart wrenching, talking with families, if your patients are able to communicate — and you’re dealing with all these deaths.
Given all of this, it’s no surprise that clinical trials can fail to recruit enough patients. A proposed RCT of hydroxychloroquine and azithromycin run by the NIH closed after enrolling just 20 patients, or 1% of their goal. I’m sure that study looked great on paper. Graveyards are full of dead RCTs and there’s research into why trials fail. The vaccine trials were unique in that boatloads of volunteers, like me, beat down the door to enter them. I am skeptical that hordes of twice-vaccinated people would be similarly eager to enter into a booster trial. Anyone who acts as if recruiting a large number of subjects into an RCT is a trivial matter while a pandemic rages is either clueless or dishonest.
- RCTs require an enormous infrastructure and multiple experts with different skills. Pfizer has this. You don’t. Most RCTs occur at multiple locations, and teams have to be in place at every site. One of the mRNA vaccine trials occurred at 152 sites worldwide. The vaccines weren’t just a scientific triumph, the RCTs were also logistical marvel. To get a sense of how complicated RCTs are, one article listed the following costs: regulatory affairs, site identification and selection, site contracting and payments, site initiation and activation, site management, onsite monitoring, drug safety management, drug logistics, biological sample logistics, clinical supplies logistics, medical writing, site close-out, project management, study files/document management, data management, statistics, quality control, communication with central CRO/sponsor, and pass-through costs, which includes, trial insurance policies for each country, shipping: physical files to sites, site contracts, and tumor/blood samples, blood tubes and shipping packages, office supplies: files, paper, and printing, payments to sites per enrolled patient (to cover clinical procedures and laboratory tests), publication fees, ethics committee evaluation fees, site contract fees, regulatory authority evaluation fees, travel costs for selection, initiation, routine monitoring, and close-out visits, central pathology and radiology reviews, translational/biomarker studies, coordinating investigators, drug manufacturing and testing, drug distribution services, EDC license and service fees, web tools (imaging platforms, eTMF), document translations, and data and Safety Monitoring Board (DSMB).
- Given their complexity, RCTs don’t always smoothly. Serious problems can sometimes arise and small hiccups are more common than not. Vaccine trials in particular have to be close to flawless. Those who enjoy spreading fear about vaccines will magnify the slightest imperfection to cast doubt on the whole project. This happened with the original COVID vaccine RCTs, much to the delight of anti-vaxxers. A rushed or sloppy RCT would do much more harm than good
- RCTs, including the vaccine RCTs, commonly exclude key segments of the population, such as pregnant women or immunocompromised patients. As such, other study designs are used to evaluate the vaccine in these populations. The exclusion of pregnant women from most RCTs is a source of controversy.
- RCT participants, who have to be savvy enough to learn about the trial in the first place, may not be representative of the general population. They are generally healthy and motivated enough to travel back and forth to the study site on a regular basis. The most vulnerable people, those who benefit from the booster the most, would likely be underrepresented in an RCT, thus skewing the results. Racial and ethnic minorities have also been underrepresented in clinical trials.
- An RCT done in one area may not generalize to another. For example, an RCT of masks in Bangladesh relied on “role-modeling by community leaders”. Its results would not be applicable to areas where community leaders oppose masks.
- Unlike any other condition in medicine, the disease being studied changes rapidly in a pandemic. The vaccine RCTs were done with a variant that is long gone. Does anyone believe these RCTs, where the vaccine was 95% effective at stopping COVID, have any relevance to our individual and policy choices today? Of course not. These RCTs rapidly became historical relics, and we’ve learned much more about the vaccines through real-world studies. An RCT of other interventions that was initiated at the pandemic’s onset, would likely be obsolete due to the more contagious variants that are circulating today.
Given this, researchers use different types of observational studies to investigate topics that are difficult or impossible to study via an RCT. Though they aren’t as rigorous as RCTs, they can provide invaluable information about vaccines/medicines once they’ve been released in the real-world.
Because they don’t select patients randomly, however, they have a greater potential for spurious associations due to random chance and confounding variables. For example, it’s possible that sicker people were more likely to get vaccinated than healthy people, who were misled into believing they had zero risk from the virus. Without controlling for this discrepancy, simply evaluating outcomes in vaccinated and unvaccinated individuals would make the make vaccine appear less effective than it actually is.
Researchers try to control for bias and most acknowledge their limitations in their papers. While these limitations can be magnified out of proportion by those who wish to cast doubt on the validity of studies whose outcomes they don’t like, there are a lot of really bad observational studies out there, and discussing their flaws is a major topic here at Science Based Medicine.
Methodolatry: RCT worship
Those who claim RCTs and only RCTs can provide reliable information are guilty of methodolatry, a favorite technique of anti-vaxxers. Disingenuous anti-vaxxers may pretend they would embrace vaccines if only there were an RCT showing (fill in the blank.) However, they reject the validity of existing RCTs, and it’s clear that if their proposed RCT were done, they would seamlessly shift to demand yet another.
For example, anti-vaxxers may point out there is no RCT showing that the HPV vaccine prevents cancer. This is true. The RCTs of the HPV vaccine used a surrogate endpoint, cervical intraepithelial neoplasia, which can be a cancer precursor. As HPV-related cancers take many years to develop, this outcome would not be possible to study in the time-frame of an RCT, nor would it be ethical to let people remain in the placebo group once evidence emerged of the vaccine’s safety and efficacy.
Unfortunately, methodolatry isn’t just a problem for anti-vaxxers. Just two short years ago, serious people wrote an article titled “Will HPV Vaccination Prevent Cervical Cancer?” which reviewed the RCTs of the HPV vaccine. They said that “None of the trials were designed to determine efficacy or effectiveness against cervical cancer. There were no reported cases of cervical cancer in any trials”. As such, they authors felt that,
It is still uncertain whether HPV vaccination prevents cervical cancer as trials were not designed to detect this outcome, which takes decades to develop… There are too few data to clearly conclude that HPV vaccine prevents cervical intraepithelial neoplasia grade 3.
The rebuttal to this piece was titled “Evidence of HPV Vaccination Efficacy Comes From More Than Clinical Trials”. It discussed “the huge amount of non-trial research evidence that enables most scientists to conclude that HPV vaccination will prevent most cervical cancers”. These scientists were right.
Of course, it wasn’t a great leap to surmise that if a vaccine that prevented a cancer precursor, it would also eventually prevent cancer. Indeed, there is now clear evidence from massive observational studies showing the HPV vaccine is very effective at preventing cervical cancer. Those who reject this evidence because it was not obtained from an RCT are guilty of methodolatry.
I am wary of the phrase, absence of evidence is not evidence of absence. Too often it is invoked by quacks when asked to provide evidence for their latest miracle cure. There argument boils down to, “There may be no evidence that magic beans cure cancer, but there’s also no evidence that magic beans don’t cure cancer. Therefore, I am right to sell magic beans to cancer patients.” They are fond of pretending that at some point in the future, science will properly study magic beans and their cancer-healing properties will be revealed.
Nevertheless, it is of course true that the absence of evidence is not evidence of absence. If aliens destroyed all guns and someone said one minute later “There’s no data that gun violence had decreased”, that person wouldn’t be wrong, but they’d be thinking like an anti-vaxxer and there’s nothing wise or useful about their comment. Massive RCTs are the best, but we are allowed to believe reasonable things with lesser evidence.
I’m confident a large RCT lasting 20 years could have shown the HPV vaccine prevents cancer, but there would have been a real cost of waiting. Countless millions of people are protected against HPV-related cancers because doctors used the vaccine based on very solid, but less-than-perfect data.
None of this was controversial amongst doctors previously. Only cranks, who wrote articles like “The Truth is Out: Gardasil Vaccine Coverup Exposed” and “Can Pharma Improve on Nature? HPV Vaccine vs Natural Infection“, opposed the HPV vaccine. And any doctor who said we should not use the HPV vaccine until there was an RCT showing it reduced all-cause mortality would be immediately recognized as a crank.
Things are very different with COVID.
Methodolatry: Impossible studies
Most often, anti-vaxxers protest there has never been an RCT of the entire vaccine schedule, and therefore studies showing the safety of individual vaccines are useless. “We both agree that RCTs are the gold-standard in medicine. How could anyone be against an RCT of the full vaccine schedule to settle this once and for all?”, they ask.
They’re fully aware that no parent would sign their infant up for such an RCT, nor would it be approved by an IRB. Even absent these obstacles, such a study would take decades and would be impossible to actually carry out. That’s the point.
Anti-vaxxers don’t like that studies overwhelmingly show that vaccines benefit children. So they purposefully call for impossible studies to diminish the credibility of these studies. Predictably, anti-vaxxers disparage parents who volunteer their children for RCTs of vaccines. That’s how ridiculous they are.
Anti-vaxxers are always able to move the goalposts, identifying gaps that they feel only an enormous RCT could fill. The RCTs that have been done are deemed fatally flawed. Frequently, they are felt to be too small in size or too short in duration. Though there are many studies showing vaccines are safe and effective, the only study that matters to anti-vaxxers is just one more, forever undone RCT.
However, demanding impossible RCTs while rejecting the perfectly good studies that have already been done is the entire point for those who wish to spread fear about vaccines and fetishize “natural” immunity. In contrast, when an observational study claims to reveal vaccine imperfections, anti-vaxxers suddenly have no issue with non-RCTs, even when the methods are extremely dubious. In fact, these studies are lauded as bombshells.
Image source: https://virologydownunder.com/
RCTs in a pandemic
Fortunately, there were multiple well-done RCTs this pandemic, not all of them run by pharmaceutical companies. The RECOVERY trial showed a dirt-cheap steroid saved lives in severely ill patients. They also evaluated 9 other treatments via RCTs. The researchers who demonstrated that surgical masks slowed COVID also proved that it’s possible to investigate these sort of interventions via an RCT, at least in Bangladesh where the were able to use a “grassroots network of volunteers” to gather data.
These RCTs were medical science at its best, and there absolutely should have been more of them. Hopefully before the next pandemic, the CDC will have established an “RCT Strike Force” that is capable of rapidly testing interventions. Citizens also need to know that signing up for RCTs is a heroic and vital effort where their safety is a priority. Without these brave volunteers, medical progress would stop.
Everyone who worked on or volunteered for an RCT this pandemic deserves our gratitude. It was really hard work.
Though I wish more interventions had been studied via enormous RCTs, I recognize that we can’t study every intervention this way. Sadly, we don’t have an RCT Strike Force today, so our public health leaders had to make choices. You may disagree with their choices, but they couldn’t have studied everything via an RCT despite what some contrarian doctors claim. Moreover, there is an opportunity cost. Every dollar and hour spent running an RCT for boosters would be a money and time not spent convincing people to get the first two doses.
It’s not easy to say exactly which interventions can and should be studied via an RCT in a raging pandemic. They are necessary to properly evaluate new vaccines. I’m glad that this was our top priority. They are necessary to properly evaluate medications. I didn’t give my COVID patients hydroxychloroquine or ivermectin based on a few lousy, even fraudulent, observational studies. Without a well-done RCT showing otherwise, except for patients facing certain death, I assumed these drugs would result in more harm than benefit.
But other interventions have an entirely different risk/benefit profile and favor their use even absent large RCTs. We often have to do our best with solid but imperfect data obtained via observational studies or small RCTs. Early in the pandemic, decisions had to be made with no data at all. Such is life. Time is not an unlimited luxury in a pandemic and we can’t let perfect be the enemy of good when forklifts are needed to move dead bodies to overflowing morgues. As Dr. Trisha Greenhalgh wisely wrote:
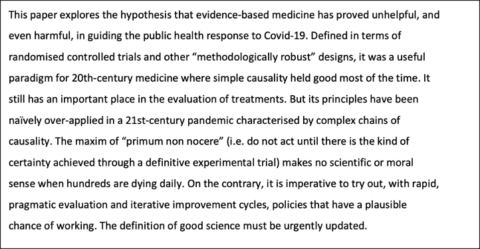
Regulators were right to have suggested a booster without the benefit of an RCT
Circling back to boosters, the evidence we have about their value isn’t perfect, but it’s very good. An RCT of 10,000 people showed that a booster was safe and 95% effective at stopping COVID. Predictably contrarian doctors minimized this trial saying there was “no data” the vaccine prevented hospitalizations and deaths. This is true, but like those who claim there’s no evidence that the HPV vaccine stops cancer, it’s not wise or helpful. In fact, it’s potentially dangerous. There are a lot of people who don’t know how much the third shot could help them.
Of course, it wasn’t a great leap to surmise that if vaccine stopped COVID infections, it would also lower COVID hospitalizations and deaths. Indeed, there is now clear evidence from large observational studies in different countries showing that boosters are effective at limiting severe disease. Additionally, vaccines still help stop the spread of the virus. Again, we are allowed to believe reasonable things.
Furthermore, the risks were not that high. Had boosters been of no benefit, the worst case scenario would have been an unnecessary vaccine dose for millions of people. This is problematic given the serious issue of vaccine inequity, but hardly a tragedy for those who received the vaccine. Fortunately, the vaccine-myocarditis rate is much lower with the booster and patients almost always do well in a short time.
I’m sure that if regulators could have snapped their fingers and willed a massive booster RCT into existence, they would have. Since they don’t operate in Fantasyland, they had to make a decision based on the best evidence they had at the time.
Had they demanded an RCT large enough to show the booster prevented hospitalizations and deaths, we might just now be getting the results, assuming enough people volunteered to let it be run at all. Remember, an NIH trial at the start of the pandemic closed after enrolling just 20 people, though it “planned to rapidly enroll approximately 2,000 adults”.
Moreover, a booster RCT that started last summer, would have begun before the arrival of variants that are more contagious and seem better at evading the immune system. It’s not clear that its results would any more relevant today that the RCTs of the first two doses.
Regulators were clearly right to have suggested boosters without the benefit a massive RCT. Many millions of people would have been left vulnerable while a booster RCT was run. Doctors who actually treat COVID patients know that this delay would have been very costly and the information gained would have been barely of use.
Currently, the main issue with boosters is that most people are convinced they don’t need one. This is not a surprise. Even after an RCT showed the booster was extremely effective in preventing COVID, contrarian doctors thought it was really funny to sit together in a podcast studio and proudly declare they were “unmasked, unboosted, and unrepentant”. One joked that being an “unboosted male” was his preferred pronoun. They were not discussing the results of a massive RCT showing the booster failed, of course. They require massive RCTs to advocate for vaccines, but they don’t require any evidence at all to trash them. They presumed that because there wasn’t a massive RCT showing the booster prevented severe COVID, that meant the booster didn’t prevent severe COVID. For these doctors, absence of evidence is evidence of absence.
Doctors unconcerned with pandering to their podcast audience – those who actually treat COVID patients – know the best way to save lives and prevent suffering is to encourage every eligible person to get a booster, not to spread unwarranted doubt about the solid evidence we have that they are beneficial. While some contrarian doctors have belatedly done this for the most vulnerable adults, boosters have been shown to be of benefit for every age group studied thus far, even teens.
Perhaps more people would have taken this crucial dose if influential doctors hadn’t made a public mockery of it all, punching down at vulnerable people for giggles.
A blatant double standard
Contrarian doctors are very familiar with the strengths and weaknesses of various study designs, and they could have used their large platforms to educate the public on this topic. They could have informed people that while all doctors agree RCTs are the gold-standard, having an idea for an RCT is infinitely easier than actually doing an RCT.
Instead, they’ve mislead their audience into believing that only enormous RCTs can determine the value of pandemic interventions, that enormous RCTs are trivial endeavors, and that more enormous RCTs weren’t done because the folks in charge were stupid and apathetic. In so doing, they successfully undermined confidence in all measures (vaccines, masks, testing, lockdowns) to control the virus and public health in general.
One doctor even proposed that no public health restriction last longer than three months unless it can be proven beneficial in an RCT. I guess restaurants will have to get rid of their bathroom signs saying Employees must wash their hands before returning to work, unless an RCT can prove this is beneficial by August. The guy making your pizza can determine his “own personal risk level” the next time he uses the bathroom at work. After all, there’s “no data” he’s doing anything wrong, is there?
The gimmick becomes entirely clear when one realizes the blatant double standard they have for when data is deemed reliable. Those doctors who call for an RCT for every proposed measure to limit the virus are perfectly content to use weak observational data, or no data at all, when it bolsters their argument that children should be left vulnerable to the virus. Though information on vaccine side-effects comes mainly from observational studies, contrarian doctors discuss this topic all the time. They’ve not questioned the validity of this data because it did not arise from RCTs. It’s only with purported vaccine benefits that the rigor of an RCT is demanded.
As with the booster trial, even then RCTs are often deemed insufficient. The pediatric RCTs (here and here) showed the vaccine was extremely effective in preventing COVID. However, in their missives opposing pediatric vaccination, contrarian doctors either pretended these studies didn’t exist or they blatantly misrepresented them, falsely claiming they didn’t measure “clinical outcomes”. They disparaged their usefulness, saying they were too small to “inform the safety of a vaccine that will be given to many millions”. Another doctor said, “There are no RCTs that show the vaccine prevents deaths or provides any other tangible benefit to children, while there could be harms”. For doctors sheltered from the consequences of their words, positive facts about the vaccine, even when from an RCT, are unmentionable facts.
Of course, it wasn’t a great leap to surmise that if a vaccine stopped COVID infections, it would also lower COVID hospitalizations and deaths. Indeed, there is now clear evidence from many observational studies showing that the vaccine is very effective in preventing these rare but devastating outcomes in children. But because these weren’t RCTs and they show the vaccine is beneficial, contrarian doctors do their best to pretend they don’t even exist. They actively resist believing reasonable things.
An impossible study
Despite the copious evidence, from both RCTs and real-world studies, that the vaccine benefits children, predictably, contrarian doctors feel yet another RCT is needed. Just last week, a contrarian doctor said,
If Pfizer and Moderna want these vaccines to be given to children, they should first conduct a randomized controlled trial that shows that they reduce hospitalization and all-cause mortality. They failed to do so for adults. They should not get away with that for our children.
I am going to do something that will likely come as a huge surprise to this doctor. I am going to pretend he was serious. I encourage you to do the same the next time a doctor suggests an RCT. Consider whether the proposed study would really change anything and whether or not that study could really be done. At first glance, his demand seems reasonable. It would be nice to have an RCT showing that the vaccine saves children’s lives.
So, would it actually be possible to run this RCT?
Fortunately, children rarely die from COVID or anything else. A child dying in a vaccine RCT would be an exceedingly rare event. As such, it would take one of the largest and longest RCTs in the history of medicine to evaluate the vaccine’s effect on all-cause mortality. As such, this trial requires an immense number unvaccinated children whose parents would be willing to enter them into an RCT with a 50% chance they would get vaccinated.
LOL, as they say.
There are many more obstacles. Would an IRB approve a study where children are purposefully left unvaccinated? Of course not. Would ethical doctors work for this study or enroll their patients in it? Of course not. Would anyone fund it? Of course not. Even if these obstacles didn’t exist, would the results be available in a useful timeframe? Of course not.
As with anti-vaxxers calling for an RCT of the entire vaccine schedule, there’s no way this study could actually be run. It’s just another impossible study. Again, that’s the point. Calling for a bevy of RCTs, with no regard as to whether they could actually be done, is what contrarian doctors do when they don’t like the results of the many studies showing the vaccine is beneficial for children.
This willful blindness makes some sense when one realizes the individual demanding this impossible RCT was one of several influential doctors who wanted unvaccinated children to contract COVID. His efforts were very successful. He should take a public victory lap.
Instead, after 1,500 dead children died and tens of thousands more hospitalized, he’s beclowning himself to avoid acknowledging the overwhelming evidence the vaccine can lessen these severe outcomes. He can’t point to any actual evidence the vaccine is riskier that the virus. All he can do is wish away unwanted studies, demand an absurd RCT, and loudly proclaim that until this undoable study is done, there’s literally no evidence in the world that could convince him children should be protected from a potentially deadly virus. All he’s got is methodolatry, and he’s happy to leave children vulnerable to COVID rather than say “I was wrong”.
Though this impossible RCT is an unserious demand from an unserious person, it has a very serious effect – it fools parents into believing the pediatric vaccine hasn’t really been tested, when nothing could be further from the truth. Thanks in part to this and many other falsehoods spread by contrarian doctors, pediatric vaccine rates are abysmally low.
It’s not just Pfizer and Moderna who want these vaccines to be given to children, as this doctor suggested. Essentially all doctors who actually care for sick children want them vaccinated too. They have to deal with the real-world consequences of myths spread by contrarian doctors. The pandemic has been about much more than making YouTube videos on their laptop for many pediatricians.
Doctors who call for an RCT for everything, generally haven’t run a single RCT on anything
And suddenly I have déjà vu. This sort of sophistry is very familiar to those of us who thought it was worthwhile to think about these issues prior to the pandemic. It’s all just pathetic variations of “Will HPV Vaccination Prevent Cervical Cancer?” blended with a dose of “Can Pharma Improve on Nature? HPV Vaccine vs Natural Infection”.
Contrarian doctors are always able to move the goalposts, identifying gaps that they feel only an enormous RCT could fill. The RCTs that have been done are deemed fatally flawed. Frequently, they are felt to be too small in size or too short in duration. Though there are many studies showing vaccines are safe and effective, the only study that matters to contrarian doctors is just one more, forever undone RCT.
However, demanding impossible RCTs while rejecting the perfectly good studies that have already been done is the entire point for those who spread fear about vaccines and fetishize “natural” immunity. In contrast, when an observational study claims to reveal vaccine imperfections, contrarian doctors suddenly have no issue with non-RCTs, even when the methods are extremely dubious. In fact, these studies are lauded as bombshells.
When pandemic interventions aren’t studied via an RCT, it’s not because doctors are ignorant and lazy, it’s because these studies are expensive, slow, and really hard. It’s no surprise that contrarian doctors always call for someone else to do an RCT rather than doing these studies themselves. It’s extremely easy to point a camera at yourself and bemoan that other doctors failed to run dozens of RCTs. It’s extremely difficult to actually run an RCT.
That’s why doctors who call for an RCT for everything generally haven’t run a single RCT on anything.